
Test your knowledge on Menopause by answering True or False to the following statements:
1. Menopause is a topic not widely studied in the literature, and little to nothing is taught about it in medical schools, OB/GYN residencies, or physical therapy / other health care provider educational programs.
2. Menopause is a sudden event occurring at age 51.
3. Hot flashes are the only symptom of menopause, and are experienced by all women.
4. Menopause is associated with an increased risk of osteoporosis and cardiovascular disease.
5. Hormone replacement therapy (HRT) is dangerous due to the elevated risk of cancer and other serious health issues, and should not be utilized.
6. Musculoskeletal / joint pain in a menopausal woman is age-related arthritis.
7. Society and culture idolize youth, vitality, and fertility making it easy for menopausal women to feel self- conscious, bewildered, and isolated.
So let's unpack these and see how you did.
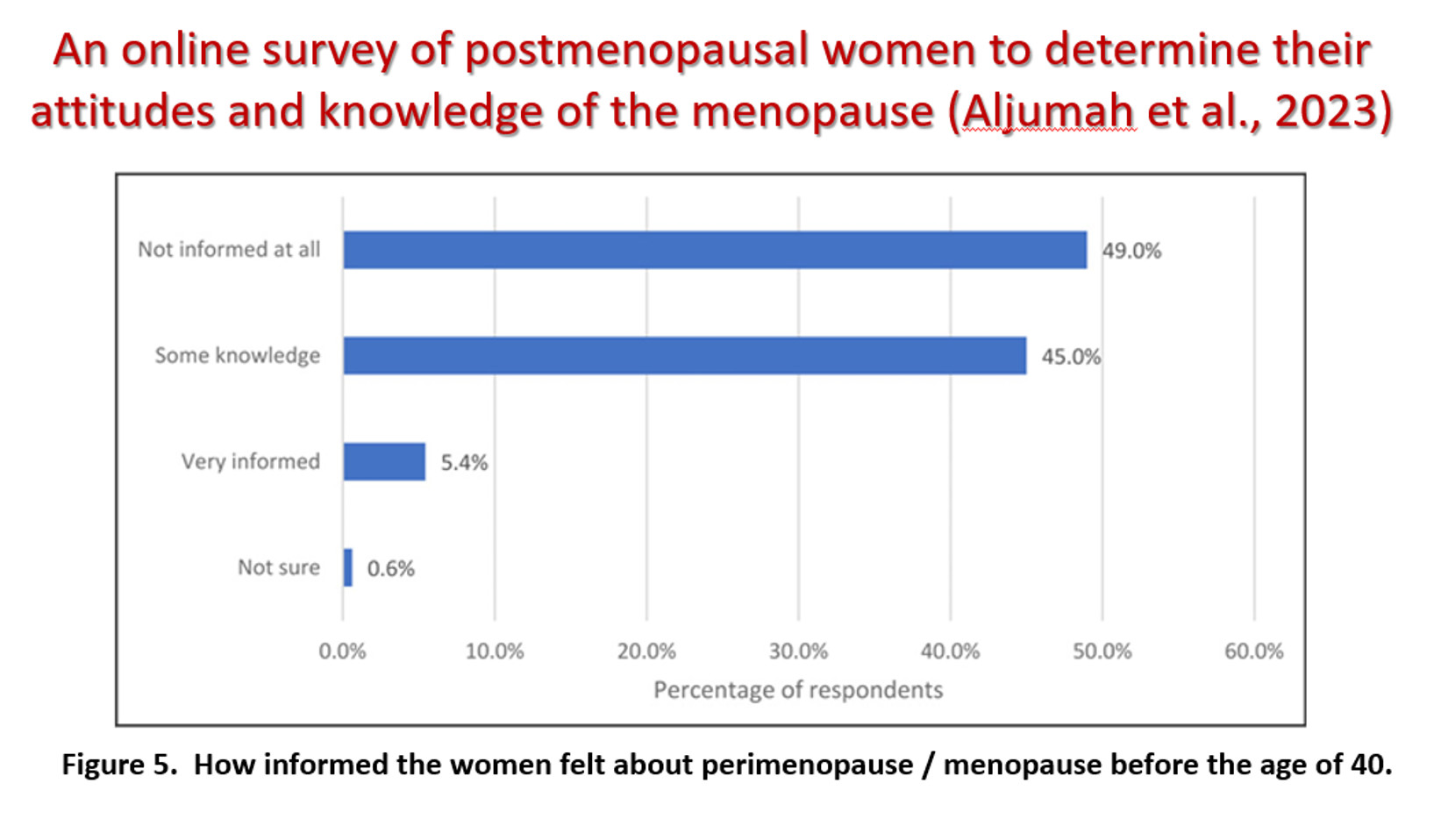
1. TRUE. Most health care provider educational programs spend little to no time learning about menopause. There is also very little research done on the topic, even though in 2025 it was estimated that 1.1 billion women worldwide were in menopause transition or post-menopausal, with 1 million in the US alone. This means that many women approach menopause with little information or understanding of the process. A 2023 UK survey of 829 post-menopausal women (see image below) asked how informed they felt about menopause before age 40. 49% said they did not feel informed at all, and 45% said they knew only a little about it. The researchers concluded that these women lacked information on the subject and also felt their healthcare providers had insufficient training, which left the women feeling unsupported and unprepared.
2. FALSE. Menopause is a process of gradually declining ovarian estrogen production that can last 5-10 years, hence the terms perimenopause or menopause transition. The average age for completion of this transition is 51 but some women are older and some younger, with race being an influential factor. Technically, menopause is the term for the cessation of the menstrual cycle for 12 consecutive months. So if a woman skips her cycle for 9 months then has a period she is more correctly in perimenopause or menopause transition. After the 12th month without a period a woman then enters the post-menopausal time. If you think about it cumulatively, a woman may spend a significant portion of her life in this entire process, which varies greatly for each person.
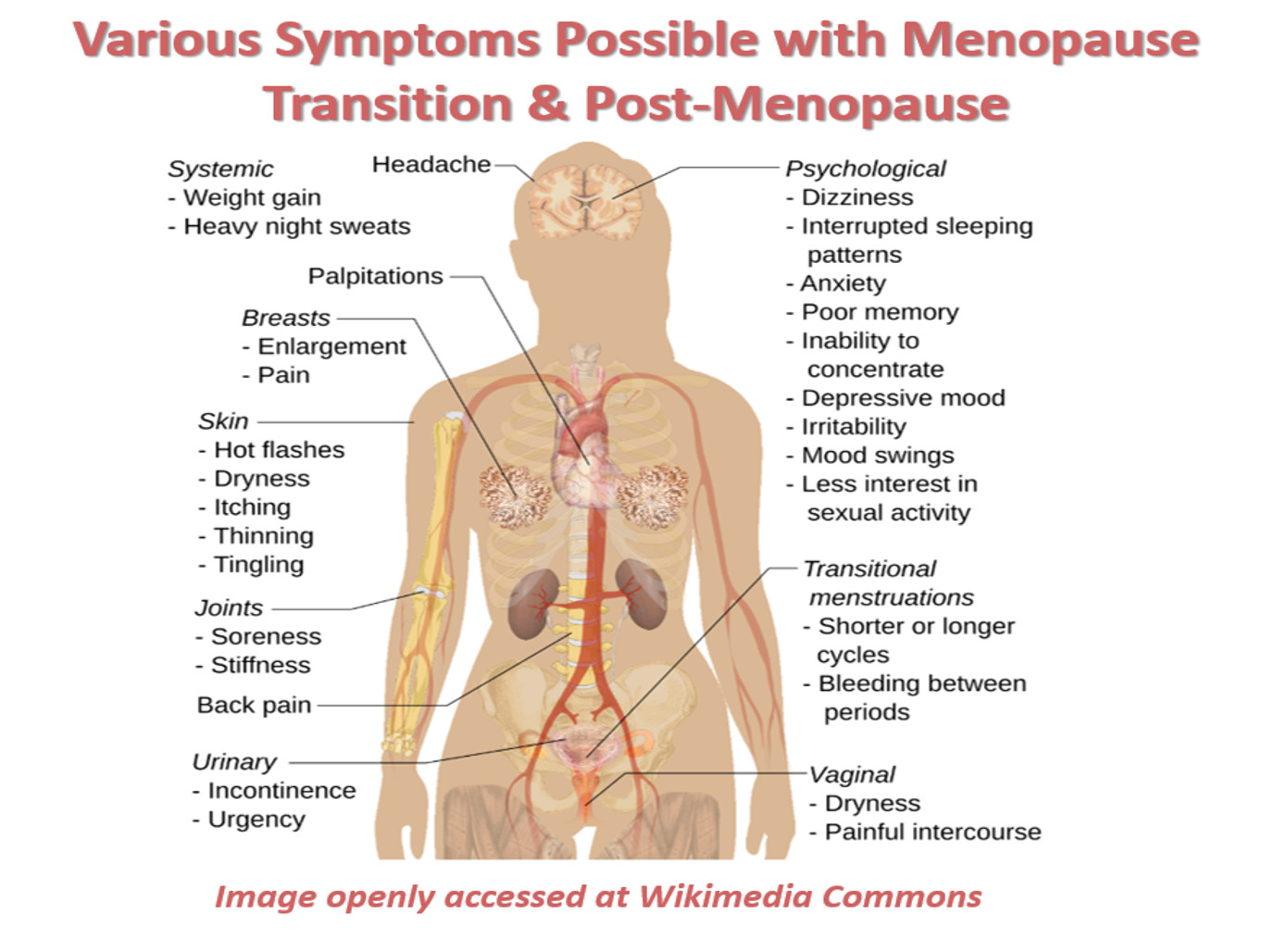
3. FALSE on several levels. First, not all women experience hot flashes (termed vasomotor symptoms [VMS]), although they do occur in ~ 80% of women. The intensity can vary from being merely bothersome to life-altering, especially when they disrupt sleep. Reduced estrogen levels can interfere with the brain's temperature control. But a less-talked-about culprit is dysfunction of the fascia impacting the circulatory system, which plays a huge role in thermoregulation through vasodilation / vasoconstriction. Additionally, abnormal metabolism and storage of fat (adipose) can also play a role in hot flashes since adipose is an insulator.
Hot flashes are certainly not the only symptom of menopause. There can also be an exacerbation of familiar as well as new aches & pains, loss of energy, mood changes, sleep disturbances, difficulty concentrating, depression, genital / urinary symptoms, digestive issues, weight gain, headaches, and more. Estrogen helps maintain the health and resilience of brain cells, and also regulates how neurotransmitters such as serotonin, dopamine, and acetylcholine function. Declining estrogen levels influence access to these essential neurotransmitters impacting cognition, mood, and pain perception.
4. TRUE. Women can lose up to 12% of bone mass during the menopause transition. This is because estrogen plays a very crucial role in bone remodeling by inhibiting the breakdown of old bone and facilitating the formation of new bone. So declining estrogen levels disrupt this crucial balance leading to a decline in bone mass, which can progress to osteopenia and osteoporosis.
As for cardiovascular health, estrogen plays a protective role with relaxation of blood vessels, normalizing cholesterol levels, reducing buildup of vascular plaque, and enhancing the presence of nitric oxide which helps blood flow. So declining estrogen levels reduce these positive influences, which is why cardiovascular disease increases in post-menopausal women and is the number one cause of death for women in the US.
5. FALSE. Hormone replacement therapy (HRT) with estrogen was first introduced in 1941 and widely used in various forms to aid in the management of menopausal symptoms. Its popularity declined abruptly in the late 1990's when reports surfaced of increasing endometrial cancer in estrogen users. Over the years the use of estrogen fluctuated and debate over its safety continued, with conflicting research presented. Then in 2002 the Journal of the American Medical Association published a study by the Women's Health Initiative citing serious risks associated with HRT. However, the study was flawed, largely based on the age and pre-existing health issues of the subjects studied. Nonetheless, HRT carried a black box warning on all prescriptions citing increased risk of heart disease, stroke, breast cancer, and blood clots with use. Multiple studies performed later showed the opposite, especially with the use of estrogen cream applied locally to the vaginal tissues. Regardless of the science showing its safety and benefits, these warnings and fears persisted until the FDA finally reversed its position and removed the warnings on all estrogen prescriptions as of November 2025. Research shows that topical localized vaginal estrogen cream is very safe due to low levels of hormones entering the blood stream. Systemic use of hormones (oral or transdermal) has been shown to be beneficial for most perimenopausal women by limiting bone mass loss. While generally safe for most women, personal health history and varying symptoms require an individualized approach to determine dosage, delivery, and appropriateness of use.
6. FALSE. More than half of perimenopausal women report pain attributed to the joints. Yet very often imaging reveals no structural changes. Menopause transition can begin in some women fairly young – far before the onset of arthritis. Estrogen aids in the mediation of inflammation, so its decline sets the stage for increased buildup of inflammatory cells. Consider too that fascia is loaded with estrogen receptors which are very subject to hormonal fluctuations. Many women enter into the menopause transition with pre-existing pains that are not at all arthritic, but are aggravated further by the changes happening throughout the body. This is good reason to address these aches and pains before they become chronic, promote compensations, and the other changes of menopause begin.
7. TRUE. But it doesn't have to be this way! As understanding of menopause expands, so do conversations about it and options for navigating it. No woman should have to endure menopausal symptoms and comorbidities in silence, bewilderment, and distress. To learn more about how fascial work may help menopause symptoms you can give me a call, send a text, book an exploratory session, or schedule a consult. You can also join me for my Menopause Seminar Saturday, February 21, 2026 from 10 a.m. to 12 noon, located at the Dancing With Karen studio in Harrisonburg, VA. There is no charge for attending, but space is limited. You can REGISTER HERE, and you can also WATCH MY SHORT VIDEO below explaining more about the seminar.
You have options - act on them!
Wishing You Health & Joy!
Colleen
Colleen Whiteford
Contact Me

.jpg)