
Gastroesophageal reflux disease (GERD) is the most common gastrointestinal diagnosis rendered by physicians in outpatient settings, with a prevalence rate up to 20%. Yet while frequently diagnosed, the utility and accuracy of many tests to confirm the actual presence of GERD is low, placing much emphasis on symptom reporting. Further complicating matters is the variability in symptoms and presentation noted throughout the literature. Most definitions cite the presence of acidic gastric contents being regurgitated upwards into the esophagus, which can harm the esophageal lining over time and predispose to ulcers, cancer, tooth/gum disease, and Barrett’s esophagus. Other symptoms may include heartburn, chest pain, difficulty swallowing, coughing, burping, frequent throat clearing, and even nausea/vomiting. The most prevalent theoretical cause is dysfunction of the lower esophageal sphincter (LES) allowing gastric juices to migrate retrograde. Other proposed factors are being overweight, smoking, ingesting large amounts of food or liquid, or consuming foods high in spices, fats, or processing chemicals. Yet the presence of any or all of these does not always result in GERD, calling into question indisputable cause and effect.
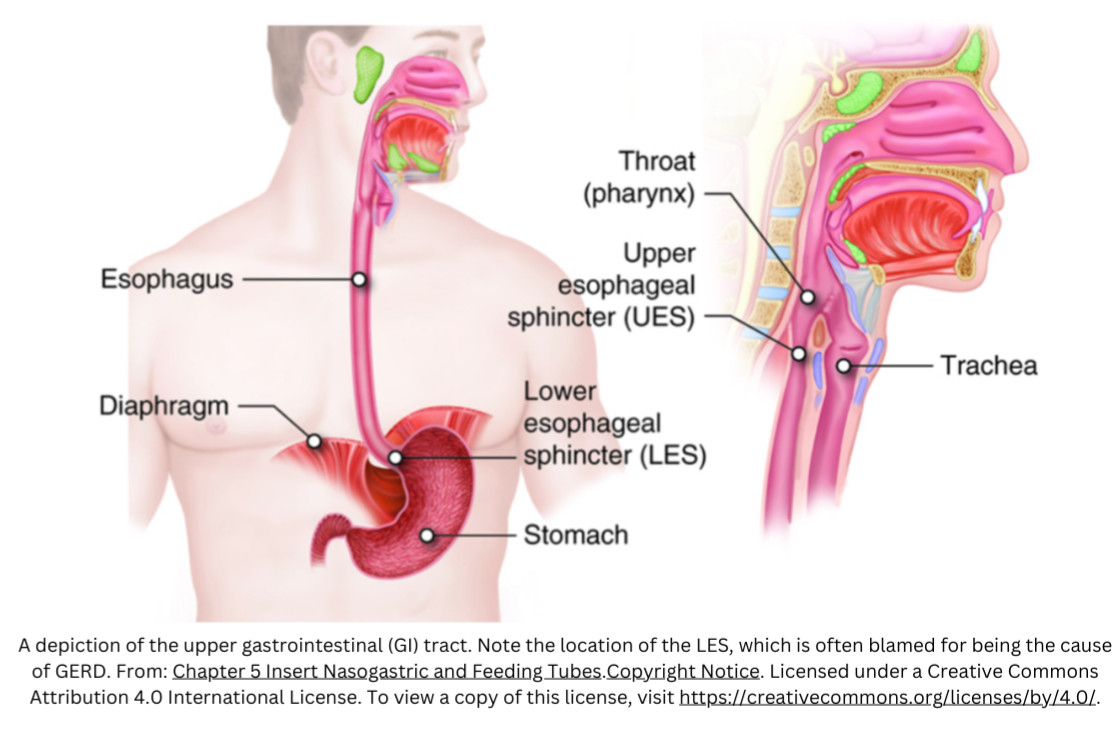
The esophagus is a muscular tube running from the throat to the stomach, and both the esophagus and stomach are encapsulated by a fascial network embedded with nerves from the autonomic nervous system (ANS) – the part of the nervous system not under voluntary control. The ANS embedded in the fascia oversees the smooth downward movement of food and beverage from the mouth to the stomach through a series of coordinated muscle contractions called peristalsis. Both the upper esophageal sphincter (UES) and the LES are circular bands of muscle in the esophagus also under the control of the ANS. When eating and drinking the Vagus (parasympathetic) innervation causes these sphincters to relax allowing normal peristalsis. At all other times there is a resting basal tone in the sphincters which closes the esophagus, courtesy of the Splanchnic (sympathetic) nerves. This prevents the retrograde movement of food/fluid, even when lying flat, burping, or cartwheeling. The only time the LES should allow retrograde movement of the stomach contents into the esophagus is with forced ejection, triggered by the nervous system when it detects something in the stomach potentially threatening to homeostasis such as poison, bacteria, or a virus. So in the absence of these threats why does the LES allow GERD to happen? Ultimately, the research and literature are inconclusive.
There are multiple measures recruited in the management of GERD. One popular approach utilizes a variety of medications which quell symptoms, often by decreasing the quantity of gastric juices secreted in the stomach for digestion. Yet time and research show that long-term use of many of these substances can have undesirable side effects (fractures, vitamin deficiencies, and infections). Another strategy is to avoid lying flat, using gravity to compensate for faulty sphincter function. Modifying food and beverage intake, amount, and schedule may also diminish symptoms. While potentially helpful, these strategies do nothing to actually address the cause of GERD leaving the problem masked but unresolved. Some sufferers resort to surgery, with very mixed results.
One explanation not often considered behind LES malfunction and GERD is fascial dysfunction. Loss of slide in the fascial layers, termed a fascial densification, can disrupt the ability of the nervous system to coordinate a smooth, voluntary or involuntary contraction in any muscle. In the case of GERD, a fascial densification can interfere with the ability of the ANS to coordinate peristalsis and appropriately relax or contract the sphincters. If the LES is not being properly signaled by the ANS to contract and remains relaxed even when peristalsis is not occurring, then it’s conceivable that stomach contents could move retrograde with something as simple as lying down, bending over, or eating a large meal. For others certain foods or beverages may trigger this abnormal sequence of events. It’s logical that fascial densification in the vicinity of the esophagus or stomach could cause this problem. But due to the continuous nature of the connective tissues, densifications contributing to GERD could be more remote, such as in the shoulder, neck, arms, or even hands. Abnormal forces and tension can be transmitted from a distance in the trunk or limbs, and exert their impact on the LES manifesting as GERD or other symptoms. This anatomical continuum necessitates assessment and treatment holistically, and may include attention to fascial densifications throughout the body stemming from old injuries, surgeries, fractures, and past problems that seem to be resolved.
I hope you can see the possibilities for changing GERD instead of masking it. To learn more about how fascial work may help you can go to my website at colleenfascialpt.com. Please feel free to give me a call, send a text, book an exploratory session, or schedule a consult. You have options – act on them!
Wishing You Health & Joy,
Colleen
References:
Kahrilas, P. J. (2008). Gastroesophageal reflux disease. New england journal of medicine, 359(16), 1700-1707.
Katz, P. O., Dunbar, K. B., Schnoll-Sussman, F. H., Greer, K. B., Yadlapati, R., & Spechler, S. J. (2022). ACG clinical guideline for the diagnosis and management of gastroesophageal reflux disease. Official journal of the American College of Gastroenterology| ACG, 117(1), 27-56.
Lacy, B. E., Weiser, K., Chertoff, J., Fass, R., Pandolfino, J. E., Richter, J. E, & Vaezi, M. F. (2010). The diagnosis of gastroesophageal reflux disease. The American journal of medicine, 123(7), 583-592.
Moayyedi, P., & Talley, N. J. (2006). Gastro-oesophageal reflux disease. The Lancet, 367(9528), 2086-2100.

.jpg)
.jpg)
